



Why is it so hard to put better mental health policies in place? Part IV
The last of a four-part series of posts on what it takes to make mental health reform a reality, plus recommendations on where to focus our efforts.

Since last post, a lot has happened in our country. From Atlanta to Boulder, families have lost loved ones and entire communities have experienced a whole new set of traumatic events – traumatic events that will only be laid on top of the other traumas all of us have experienced in the last year.
It’s hard to see some of these headlines, chyrons, and to hear the updates about these senseless tragedies. So in response, we have already and will inevitably continue to hear pleas for change – everything from addressing gun violence to finding ways to tackle racism.
All of these are important cries to for us to do something, to make a policy change. And because of the nature of these atrocities, many of them will be accompanied by cries to make policy changes that do more to improve mental health. However, as so many have written, mental health and gun violence are not issues that directly connect. If they do, gun violence is usually self-inflicted, e.g. suicide, or it’s because the person with the mental illness is a victim of/witness to someone else’s violence. We can’t blame our way out of this one:


Plain and simple, these recent tragedies are just another example of how our nation has failed to take meaningful action on things that matter – things that might not directly be related to mental health, but that we all could benefit from nevertheless.
Where mental health is concerned, I’ll pick back up with this series’ fourth and final post on policymaking. As promised, I’ll start by sharing some proof that mental health is low on our national leadership’s totem pole, but end things on a good note with recent mental health policy victories and state bills you might want to keep an eye on – or, now that you’ve read this series, recreate in your own community.
MARGINALIZATION BY THE NUMBERS
In one of my very first posts, I talked about how we got to where we are today by way of few contributions to mental health from our nation’s past presidents. Exceptions to that trend were Harry Truman, John F. Kennedy, Lyndon B. Johnson, Jimmy Carter, George W. Bush and Barack Obama – the majority of whom are all Democrats.
Since Democratic presidents have historically led the charge on mental health – though I do want to be clear that mental health is a bipartisan issue, and one that I know many Republicans do care about – I thought it would be interesting to take a look back at what conversations about mental health happened during the most recent Democratic debates. With all those Democratic leaders in one room, mental health had to come up at least a few times, right?
Wrong.
Of the approximately 30 hours they spent debating, according to the transcripts, the 2020 Democratic presidential candidates spent roughly five minutes talking about mental health. Five minutes out of ~1,800 total minutes. Not even a full percentage point.

Why do you think that is? If it’s something they likely deem as important, why wasn’t mental health something that any of the presidential candidates strongly campaigned on?
Well, campaigns cost money. And remember last week when I mentioned special interest groups and their influence on politicians’ priorities? Special interest groups have got money.
Per the nonpartisan nonprofit Center for Responsive Politics:
· Health professionals – who could potentially lose patients to other providers if coverage for mental health care was on par with coverage for physical health care – contributed $220,625,204 in 2020.
· Insurance companies – who under the same circumstances would be forced to spend more money on their beneficiaries’ behalf – contributed $122,726,276 in 2020.
· And hospitals – who don’t see mental health as a lucrative service for them to provide – contributed $117,102,895 in 2020.
There’s no special interest group for mental health, per se, and trust me when I say that contributions by organizations solely devoted to mental health pale in comparison to these numbers.
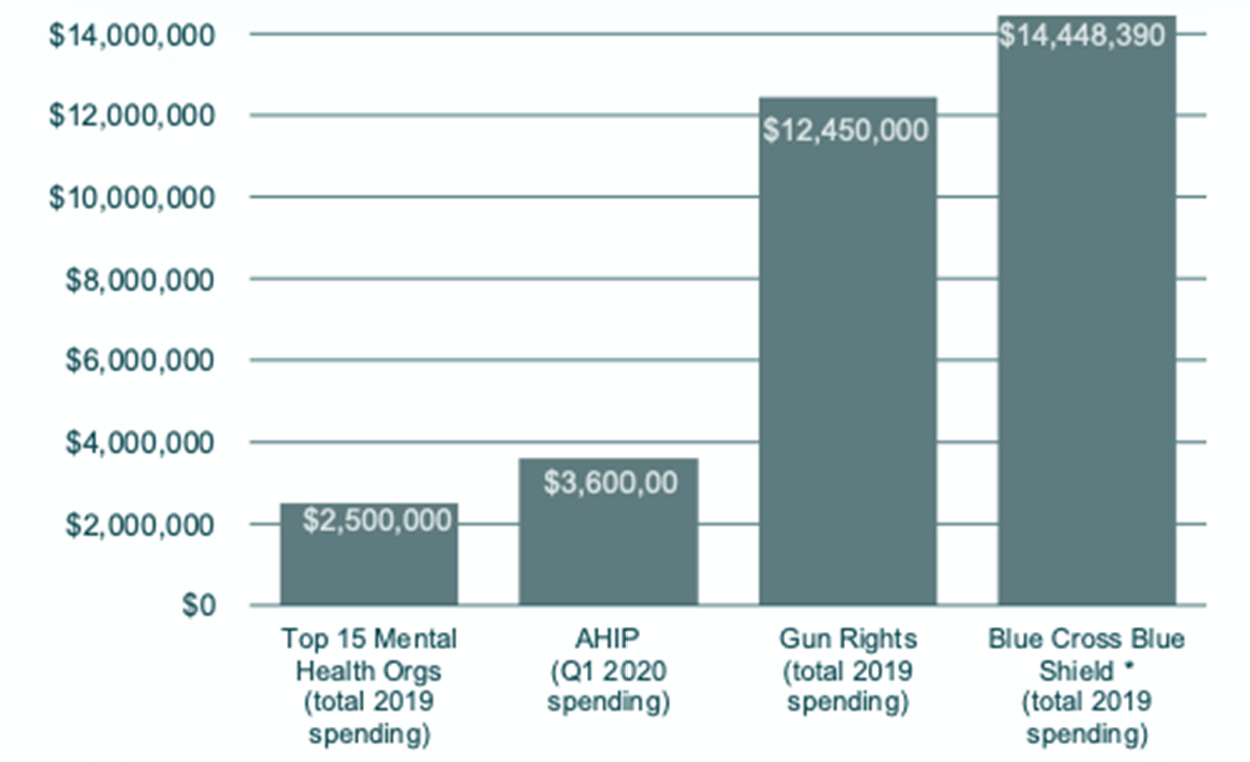
Inseparable, a new mental health policy/advocacy organization, culled through the 990s of the top 15 mental health organizations and found that they were outspent substantially - as you can see in the below graph.
In fact, according to Inseparable, in 2019 America’s Health Insurance Plans (AHIP), which is the national association representing health insurance companies, spent almost double the total amount the mental health field spent all year in just the first quarter!
STATES ARE THE SWEET SPOT
OK, so the numbers might not be in mental health’s favor at the national level, but don’t lose hope just yet. With enough of us banding together to put better mental health policies in place community by community, state by state, we will one day see sweeping mental health reform.
We are already off to a great start. For example, this past fall, California Gov. Gavin Newsom signed into law S.B. 855, a bill that requires insurers to make medical necessity determinations consistent with Generally Accepted Standards of Behavioral Health care – previously, the California Parity Act only required insurers to cover just nine mental health conditions – and ensure Californians receive coverage for care needed to treat any mental health and/or substance use disorder. And Illinois is already following suit with a campaign using the model legislation set forth by California – and it’s a snazzy campaign to boot.

Though these are only three, many more bills stand ready to join them:
· In Florida two similar bills, SB 1024 and HB 701, seeks to create a system through which complaints about mental health coverage and access to care and mental health coverage and access to care, respectively, can make their way into a report reviewed by the Governor. HB 701 was reported out of the Health and Human Services Committee on March 18, and SB 1024 had a hearing yesterday (3/24/21).
· In Georgia, SB 80, which seeks to change prior authorization rules for health care services that include treatment of mental health and substance use disorders, passed the state Senate earlier this month.
· In Texas, a bill (HB 2595) calling for the creation of mental health parity educational materials and training, a complaint portal for parity violations, and a month dedicated to “mental health condition and substance use disorder parity awareness” was just referred to the Insurance committee.
How can you help these bills move forward, or create something similar so that your community could soon benefit too? At this point, I think you already know the answer!
This concludes our series on what it takes to put better mental health policies in place, but definitely not posts about bills worth watching and a mix of mental health setbacks and successes. Keep following along for more and doesn’t hesitate to share your thoughts on what you want to see next.
Until next week, be well.